Table of Contents
This post tackles a critical topic for many readers: when and how to discontinue Prolia (Denosumab). With insights from Dr. Janet Rubin, a distinguished endocrinologist and bone biology researcher at the University of North Carolina Medical School, we’ll guide you through the complexities of Prolia discontinuation.
I will use the terms Prolia and Denosumab interchangeably in this post. They both refer to the same medication. One is the commercial name (Prolia) and the other is the clinical name (Denosumab). Although I do not use the term in this post, you will also find references to the generic version of Prolia elsewhere on the internet. The generic name is Xgeva.
Before we get into when and how to discontinue Prolia, we need to discuss how the medication works. Let’s start with that topic first.
What is Prolia?
Prolia, or Denosumab, is a powerful antiresorptive medication for osteoporosis. It works by inhibiting a molecule called RANK LIGAND, which is essential for the formation and activity of osteoclasts—the cells responsible for bone resorption. By reducing osteoclast activity, Prolia helps maintain and potentially increase bone density. It can reduce fracture risk with limited side effects. (1)
How Prolia Works at the Cellular Level
Prolia effectively halts the activity of the osteoclasts that resorb old and damaged bone, while allowing osteoblasts to continue their work. During postmenopause, osteoclast activity increases and bone formation occurs more slowly due to a drop in estrogen levels. Prolia can rebalance this process by stopping the breakdown of bone, thus maintaining denser bones over time.
A single 60 mg injection of Denosumab is administered every six months by a healthcare provider.
Prolia and Blood Turnover Markers
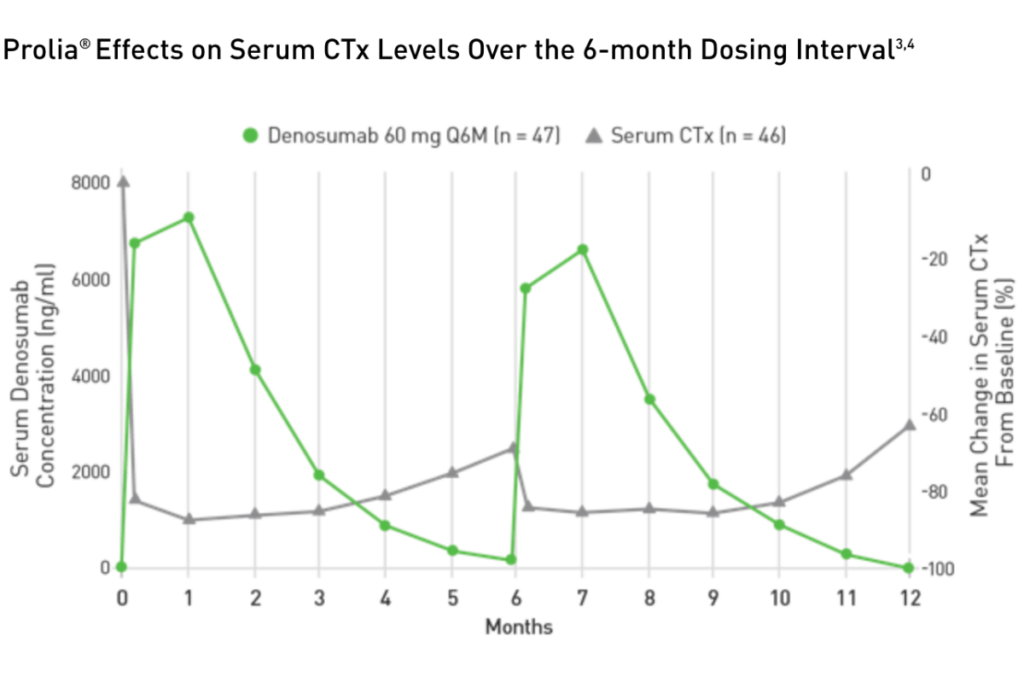
The chart below (2) illustrates how Prolia affects Serum CTx levels over one year. Serum CTx is a bone turnover marker (BTM) that measures osteoclast activity. When the CTx levels decline, as shown in the chart, this indicates a decrease in osteoclast activity. The reduced osteoclast activity, coupled with the regular osteoblast activity, increases bone density.
The chart illustrates several vital events during the Prolia treatment:
- Notice how the CTx level drops dramatically after the injection.
- As the Prolia levels in your body drop over the six months, CTx levels start to increase, indicating that osteoclast activity has resumed.
- The Prolia has largely left your body by the sixth month.
- Your physician administers a new 60 mg injection of Denosumab or Prolia, and the cycle begins again.
Your CTx level should follow a similar pattern. Suppose you have your baseline CTx level before starting Prolia. In that case, your physician can track its behavior and changes over the six months to see the effects of Prolia on your osteoclast activity.
I have had clients who have been told after two years, and a repeat bone density test, that they need to switch to another drug because they did not respond to Denusomab. They could have found this out sooner if their bone markers were monitored.
Source: Prolia website [https://www.proliahcp.com/dosing-and-administration/prolia-injection-dosing]
Bone Loss After Denosumab Discontinuation
Significant cellular changes occur when you stop Prolia. When you discontinue Prolia, osteoclasts—those bone-resorbing cells—quickly become active again. An increase in osteoclast activity can lead to an accelerated rate of bone loss, often faster than before starting Prolia, resulting in “rebound fractures.”
A 2011 study (3) examined the effects of a sudden discontinuation of Prolia with no follow-on treatment. The research found that shortly after discontinuing Prolia (and assuming no follow-on treatment), the CTX levels of the participants rapidly increased well beyond the original CTx baseline recorded before the Prolia intervention. The rapid increase in CTx levels indicated that the osteoclast activity increased and caused rapid loss in bone density in both the lumbar spine and the hip.
The study also found that within twelve to twenty-four months after the sudden stop of Prolia, the participants lost all the gains in bone density that they had made while being on Prolia treatment for two years.
The risk of spontaneous vertebral compression fracture increased in the twelve to twenty-four months after suddenly stopping the two year long Prolia treatment phase.
What causes this sudden increase in osteoclasts when you stop Prolia and do not have a follow-on treatment? We will discuss this in the next section.
Discontinuation of Denosumab: Sudden Increase in Osteoclasts
Several leading clinicians and researchers hypothesize (4) why osteoclasts rapidly increase with a sudden discontinuation of Prolia. One theory, in particular, is seen as the possible explanation.
A 2021 groundbreaking study (5) by Dr. Michelle McDonald, published in the journal Cell, revealed that osteoclasts don’t just disappear during Prolia treatment. Instead, they break into smaller pieces called osteomorphs and hide. Once a patient stops Prolia, these pieces reassemble quickly, increasing both bone resorption and fracture risk. Notably, rebound fractures occur more frequently in the spine than in the hip area.
What To Do Before You Start Prolia
There are several issues to consider before beginning Prolia. The following are some guidelines to help you decide whether to move forward with Prolia or not. Before you start Prolia:
- Book an appointment with your dentist/oral surgeon and let them know that you will soon be on Denusomab. Tell them it is a drug that you cannot get off of for several years and that the drug interferes with healing from dental extractions or implants. Do not assume they know about the complications.
- Complete any major dental work, such as implants.
- Discuss and evaluate alternative osteoporosis medications with your physician.
- Establish a baseline bone mineral density (BMD) and a serum CTX to measure osteoclast levels.
In addition, ask your physician:
- Why do they recommend intervention with Prolia, and what are their goals? Are they recommending Prolia because you have an elevated risk of fracture? Is it because they think they can get you into a lower fracture-risk zone within a reasonable time?
- How long do they think you need to be on Prolia, and what are their targets so that you can stop using the medication? Is the objective to increase bone density to offset your fracture risk? If this is your case, ask them to estimate when you will achieve that target.
- How to discontinue Prolia and transition you off of Denusomab if needed?

Bone Density, Bone Turnover and Discontinuation of Denosumab
Prolia is a very effective medication that increases bone density and reduces fracture risk. However, it is essential that you have a healthcare provider who knows how to discontinue Prolia since the discontinuation of Denosumab can present challenges that require attention and care. Health professionals, institutions, clinicians, and leading researchers have been investigating the best way to manage the use of Prolia.
For example, a working group of the European Calcified Tissue Society performed an updated systematic review (6) of existing literature on changes in bone turnover, bone mineral density (BMD), and fracture risk after Denosumab discontinuation. It provided advice on Prolia management based on expert opinion. Here is their guidance on starting Prolia treatment:
Taking into consideration that a longer duration of treatment also involves a risk of unplanned discontinuation, a very careful assessment of the indications to start Denosumab treatment in the first place should be performed, especially in younger patients, who may be at higher risk of fractures or bone loss following discontinuation. (6)
Exercise Recommendations for Osteoporosis
Exercise is an essential ingredient to bone health. I know you want to know how to discontinue Prolia, but if you have osteoporosis, therapeutic exercise needs to be part of your osteoporosis treatment program.
But what exercises should you do and which ones should you avoid? What exercises build bone and which ones reduce your chance of a fracture? Is Yoga good for your bones? Who should you trust when it comes to exercises for osteoporosis?
A great resource on exercise and osteoporosis is my free, seven day email course called Exercise Recommendations for Osteoporosis. After you provide your email address, you will receive seven consecutive online educational videos on bone health — one lesson each day. You can look at the videos at anytime and as often as you like.

I cover important topics related to osteoporosis exercise including:
- Can exercise reverse osteoporosis?
- Stop the stoop — how to avoid kyphosis and rounded shoulders.
- Key components of an osteoporosis exercise program.
- Key principles of bone building.
- Exercises you should avoid if you have osteoporosis.
- Yoga and osteoporosis — should you practice yoga if you have osteoporosis?
- Core strength and osteoporosis — why is core strength important if you have osteoporosis?
Enter your email address and I will start you on this free course. I do not SPAM or share your email address (or any information) with third parties. You can unsubscribe from my mail list at any time.
Can I Stop Prolia After One Injection?
If you’ve only had one Prolia injection, you might wonder about the risks of a rebound fracture. The longer you’ve been on Prolia, the higher the rebound fracture risk upon stopping (7). Even after a single injection, you must consult your doctor about the safest action.
According to the position paper of a working group of the European Calcified Tissue Society,
Discontinuation of Denosumab following at least two Denosumab injections carries a significant risk of a rebound effect, manifesting as considerable loss of bone mass gained during the period of Denosumab treatment and an augmented risk for (multiple) VFx (vertebral compression fracture). (6)
Dr. Elena Gonzalez Rodriguez is Deputy Chief of the Clinic in the Department of Endocrinology, Diabetes, and Metabolism at the University Hospital of Vaud (CHUV). She has investigated the effects of stopping Prolia and published several studies on that topic.
I asked Dr. Gonzalez-Rodriguez if a patient could stop Prolia after one injection. She stated that if a patient discontinues Prolia treatment after a single injection, all scientific evidence suggests no risk for biological, densitometric, or clinical (vertebral fracture risk) rebound. In a recent publication, she points out that after the second denosumab dose, there is a rebound effect with an increased risk of multiple vertebral fractures. (8)
However, if your physician recommended Prolia because of elevated fracture risk and you stop using the medication, you need to consider alternative pharmaceutical intervention to offset that risk.
Prolia Dental Work
Many aging clients frequently require dental work, including dental implants, extractions, and crowns. There is an elevated risk of dental problems, including osteonecrosis of the jaw, when people are on Prolia and have dental work. The management of Prolia during dental work demands special attention and care.
Here is some guidance from the working group of the European Calcified Tissue Society position paper on Prolia and dental work:
Regarding elective dental procedures for which treatment discontinuation is demanded by the dentist, it seems prudent to perform the procedure preferably approximately five months after the last Denosumab injection and resume treatment as soon as the lesion is healed, although this is based on expert opinion only. (6)

Vertebral Fracture Risk and Prolia
There is a greater vertebral fracture risk from stopping Prolia than in a hip fracture. According to the position paper of a working group of the European Calcified Tissue Society:
Discontinuation of Denosumab following at least two Denosumab injections carries … an augmented risk for multiple vertebral fractures. (6)
Stop Denosumab Safely
Discontinuing the use of Prolia should be done thoughtfully and under the guidance of a healthcare professional. When a patient stops using Prolia, the bone resorption process, which was previously inhibited by the drug, starts again. Bone loss may occur after stopping Prolia, and it may even happen faster than if the person had never taken the drug.
Work with your primary care provider and develop a sound plan to transition off Prolia. In many cases, patients are transitioned to bisphosphonates, which are another type of osteoporosis drug that can be taken for several years. The specific bisphosphonate used may vary depending on individual circumstances and preferences. It is essential to have regular follow-up appointments and not delay or skip doses of Prolia, as rebound fractures can occur within a couple of months of discontinuation.
Ultimately, the decision to discontinue Prolia and the choice of alternative treatment should be made on an individual basis, taking into account factors such as age, overall health, bone mineral density, and the risk of fractures. It is recommended to communicate openly and ongoing with a healthcare professional to determine the best course of action.
European Calcified Tissue Society Guidance
Here is some guidance from the working group of the European Calcified Tissue Society position paper (6) on how to discontinue Prolia:
- To limit this risk (rebound fractures), it is currently recommended either to continue Denosumab therapy or to prescribe a potent bisphosphonate when Denosumab is stopped.
- A shorter duration of Denosumab treatment (i.e., up to 2.5 years) in patients with otherwise low fracture risk could justify treatment with an oral bisphosphonate for 1 to 2 years.
- In case of previous intolerance to oral bisphosphonates, expected poor adherence, or polypharmacy, Zolendronate can be administered. Zoledronate is also known as Zoledronic acid or its trade name Zometa is a bisphosphonate that is administered by infusion. It can be given once and repeated if bone turnover is still inappropriately high.
- Patients who have been treated with Denosumab for a longer period (i.e., > 2.5 years) or who are at persistently high risk for fracture should receive Zoledronate.
- Pending results of ongoing randomized control trials on the optimal bisphosphonate regimen, bone turnover markers can provide clinical guidance on the timing and duration of zoledronate treatment.
Dr. Rubin's Insights
Endocrinologist, Dr. Janet Rubin provides valuable insight on how to discontinue Prolia. She emphasizes the need for personalized treatment plans. For younger patients, Dr. Rubin aims to transition them off Prolia after achieving significant bone density gains. For older patients, particularly those in their late eighties, she might continue Prolia without interruption due to its safety and effectiveness.
What to Take After Stopping Prolia
Transitioning off Prolia typically involves switching to a bisphosphonate, such as Zoledronic acid. This strategy helps maintain the gains in bone density and prevent rebound fractures. However, this approach can have challenges, including patient reluctance to take bisphosphonates or specific health conditions that preclude their use.
In a study on vertebral fractures and bone loss, after denosumab discontinuation (7) published in the journal Bone in 2021, Swiss researcher Dr. Judith Everts-Graber and colleagues made the following conclusions:
- We conclude that the fracture rate after denosumab discontinuation remained low in patients with subsequent antiresorptive treatment. Multiple vertebral fractures were only observed in patients without subsequent therapy.
- Zoledronate (a bisphosphonate) was associated with a lower incidence of vertebral fractures within 24 months after denosumab discontinuation.
Recent Circumstances Impacting Prolia Discontinuation
Two recent events have highlighted the importance of careful Prolia management. In Europe, some breast cancer patients who used Prolia during treatment, experienced rebound fractures upon remission and discontinuation. Similarly, during the COVID-19 pandemic, many patients missed their Prolia doses, leading to increased fracture rates and much unnecessary suffering.
Timing for Denosumab Discontinuation
The timing of the transition to bisphosphonates is critical. Rebound fractures can occur within a few months of stopping Prolia. To mitigate this risk, Dr. Rubin advises starting a bisphosphonate shortly after the last Prolia injection.
Criteria for Denosumab Discontinuation
When can you safely stop Prolia? Dr. Rubin suggests considering discontinuation once you have achieved significant bone density improvements. However, each patient’s situation is unique. Make your decisions in close consultation with your healthcare provider.
How to Discontiue Prolia: Alternative Treatments
If bisphosphonates aren’t an option after stopping Denusomab, Dr. Rubin may consider alternatives like Raloxifene (Evista) or other estrogen-like treatments. These alternatives can also help maintain bone density and reduce fracture risk.
Stopping Prolia After 5 to 10 Years
How long should you stay on Prolia if you’ve been on it for five to ten years and seen positive results? Dr. Rubin advises discussing long-term use with your doctor. The conversation should consider your overall health and fracture risk. For some patients, particularly those with specific health conditions, staying on Prolia might be necessary.
In a 2021 study (7), Swiss researcher Dr. Judith Everts-Graber and colleagues made the following conclusions:
- Younger age and longer duration of Denosumab therapy were significantly associated with higher bone mineral density (BMD) loss after Denosumab discontinuation. Thus, if Denosumab is to be discontinued, special attention should be paid to early postmenopausal patients and those who have been treated with Denosumab for long periods (>3 years). These patients require more intensive monitoring and treatment than older patients with shorter treatment durations.
- Also, patients with prevalent fractures should be treated and monitored more intensively because they are at particular risk for new vertebral fractures after denosumab discontinuation.
Exercise Recommendations for Osteoporosis
Exercise is an essential ingredient to bone health. I know you want to know how to discontinue Prolia, but if you have osteoporosis, therapeutic exercise needs to be part of your osteoporosis treatment program.
But what exercises should you do and which ones should you avoid? What exercises build bone and which ones reduce your chance of a fracture? Is Yoga good for your bones? Who should you trust when it comes to exercises for osteoporosis?
A great resource on exercise and osteoporosis is my free, seven day email course called Exercise Recommendations for Osteoporosis. After you provide your email address, you will receive seven consecutive online educational videos on bone health — one lesson each day. You can look at the videos at anytime and as often as you like.
I cover important topics related to osteoporosis exercise including:
- Can exercise reverse osteoporosis?
- Stop the stoop — how to avoid kyphosis and rounded shoulders.
- Key components of an osteoporosis exercise program.
- Key principles of bone building.
- Exercises you should avoid if you have osteoporosis.
- Yoga and osteoporosis — should you practice yoga if you have osteoporosis?
- Core strength and osteoporosis — why is core strength important if you have osteoporosis?
Enter your email address and I will start you on this free course. I do not SPAM or share your email address (or any information) with third parties. You can unsubscribe from my mail list at any time.
Management of Prolia Case Study
When Jane was diagnosed with osteoporosis, her physician recommended she take Prolia (Denosumab). Unfortunately, the management of her Prolia was not as good as it should have been and Jane experienced a number of problems. Here is her Prolia management story.
There are two major lessons from her experience:
- You should not assume that exercises you find online labelled for “osteoporosis” or for “seniors” are safe for you to do. This applies to all social media sources, even those presented by Physical Therapists. Individuals with osteoporosis need an exercise program targeted at their fracture risk; this is particularly true for individuals with compression fractures.
- If you are receiving Prolia injections, it is due to the fact that you are at an elevated risk of fracture. I have many clients who need to be on Prolia because their bone density and bone quality is so poor that a fall could lead to a catastrophic fracture. The problem is not the medication. Prolia is very effective. Problems occur when the administration of the drug is not managed as well as it should be. This is particularly true when it comes to the termination of the use of Prolia.
Here is Jane’s story.
Conclusion to How to Discontinue Prolia
The rebound effect of Denosumab on bone health has brought attention to the importance of carefully managing the discontinuation of this medication. Healthcare providers should assess an individual’s risk and work together with their patients to develop a personalized treatment plan. Regular follow-up appointments and adherence to prescribed treatments are crucial for maintaining optimal bone health and reducing the risk of fractures.
Stopping Prolia is a complex process that requires careful planning and individualized care. The insights from Dr. Janet Rubin highlight the importance of understanding how Prolia works and the risks associated with stopping it. Remember, your healthcare provider is your best resource for navigating these decisions.
Bone health is complex and highly individualized. Strengthen your relationship with your doctor to guide you through maintaining strong and healthy bones. Continue to exercise intelligently, choose foods that support healthy bones, and trust MelioGuide to help you navigate through your journey with osteopenia or osteoporosis.
Further Readings



References
- Bone, HG, et al. 10 years of denosumab treatment in postmenopausal women with osteoporosis: results from the phase 3 randomised FREEDOM trial and open-label extension. The Lancet. Volume 5, Issue 7. P513-523, JULY 2017
- Source: Prolia website [https://www.proliahcp.com/dosing-and-administration/prolia-injection-dosing]
- Bone, HG, et al., Effects of denosumab treatment and discontinuation on bone mineral density and bone turnover markers in postmenopausal women with low bone mass. Journal of Clinical Endocrinology and Metabolism. 2011 Apr;96(4):972-80. doi: 10.1210/jc.2010-1502. Epub 2011 Feb 2.
- Ferrari, S., Langdahl, B. Mechanisms underlying the long-term and withdrawal effects of denosumab therapy on bone. Nat Rev Rheumatol 19, 307–317 (2023). https://doi.org/10.1038/s41584-023-00935-3
- McDonald M. et al. Osteoclasts recycle via osteomorphs during RANKL stimulated bone resorption. Cell. 184, 1330–1347 March 4, 2021
- E Tsourdi, M.C. Zillikens, C Meier, JJ Body, EG Rodriguez, AD Anastasilakis, B Abrahamsen, E McCloskey, LC Hofbauer, N Guanabens, B Obermayer-Pietsch, SH Ralston, R Eastell, J Pepe, A Palermo, B Langdahl. Fracture Risk and Management of Discontinuation of Denosumab Therapy: A Systematic Review and Position Statement by ECTS. The Journal of clinical endocrinology and metabolism. Vol 106. Issue 1. pp. 264-281. Published – Jan 2021
- Everts-Graber. J, et al. Risk factors for vertebral fractures and bone loss after denosumab discontinuation: A real-world observational study. Bone. Volume 144, March 2021, 115830
- Lamy O., Gonzalez-Rodriguez E., et al. Stopping Denosumab. Current Osteoporosis Reports. 2019 Feb;17(1):8-15. doi: 10.1007/s11914-019-00502-4.
Comments